
Henry Aaron and Harold Pollack in The New Republic (emphasis mine):
The U.S. health-care system is far and away the most complex in the world, one that includes employer-sponsored coverage, Medicare, Medicaid, Tricare, the Indian Health Service, and small-group and individual insurance coverage—and that’s before Obamacare was implemented. Given that complexity, some on the left say, life would be simpler if only Congress had been willing—which it was not—to scrap all current arrangements and replace them with a single, federally administered health insurance plan…
We wish ACA had gone farther. It could have provided more generous premium assistance and cost-sharing for working families. It could have allowed people near retirement to buy into Medicare. Alas, senators such as Joe Lieberman—not Obama—scuttled these possibilities. The ACA is only the first step in a long journey of needed health reforms.
[Robert] Kuttner and [Nancy] Folbre are correct that Medicare for All would be much easier to understand. Perhaps, as Obama among others has said, Medicare for All would be preferable to our current system, were we designing that system from scratch.
But we aren’t. The slogan “Medicare for all” was never incorporated in a well-crafted legislative proposal. Had it been, it would have been even easier than Obamacare for Republicans to oppose. And implementation would have been formidably difficult. Had the transition to single-payer ever been specifically mapped out, it would immediately have become apparent that this process requires wholesale replacement or rewiring of employer-based coverage, major changes in the relations between states and the federal government. Hundreds of billions of dollars in transfers and new taxes would have been necessary. Enterprising constitutional conservatives surely would have identified plausible court challenges…
The backlash against the ACA is occurring because it disrupts coverage of several million people in the individual and small-group insurance market. Transition to single-payer would have been far messier, disrupting coverage for hundreds of millions of Americans, with a much larger and more explosive mix of winners and losers.
As lukewarm as I am about the ACA [see Note 1 below], I agree with Aaron and Pollack’s analysis. It’s a relatively simple thing to say “[B] is better than [A]. We should stop doing [A] and start doing [B].” Set aside the fact that we’re not anywhere close to agreeing on how best to do health care in the US, agreeing on what the best practice is the easy part. [See Note 2 below] Depending upon what you’re trying to do, getting from A to B can be extremely difficult. It may not even be feasible. As much as I believe that single-payer would be the way to go if we were starting from scratch, I’m inclined to believe that the ACA is about as good as we’re going to do given where we’re at. Forty, thirty, maybe even twenty years ago if believe a transition to single-payer could well have worked. Even if legislation got passed I think the odds of success now would be very low. As a country, I don’t believe we currently have the mindset necessary to tough it out through a messy conversion. Who knows, maybe in fifty years we will and possibility for success look good again. The country can cross that bridge if and when it comes to it. The ACA is what we’ve got now and we need to put our energy into making it work.
PS In lieu of single-payer, enjoy your $2000 stitches courtesy of your local private nonprofit hospital and, if you’re fortunate, covered by your health insurance plan. And you wondered why your premium is $500/month?
PPS Don’t forget this:
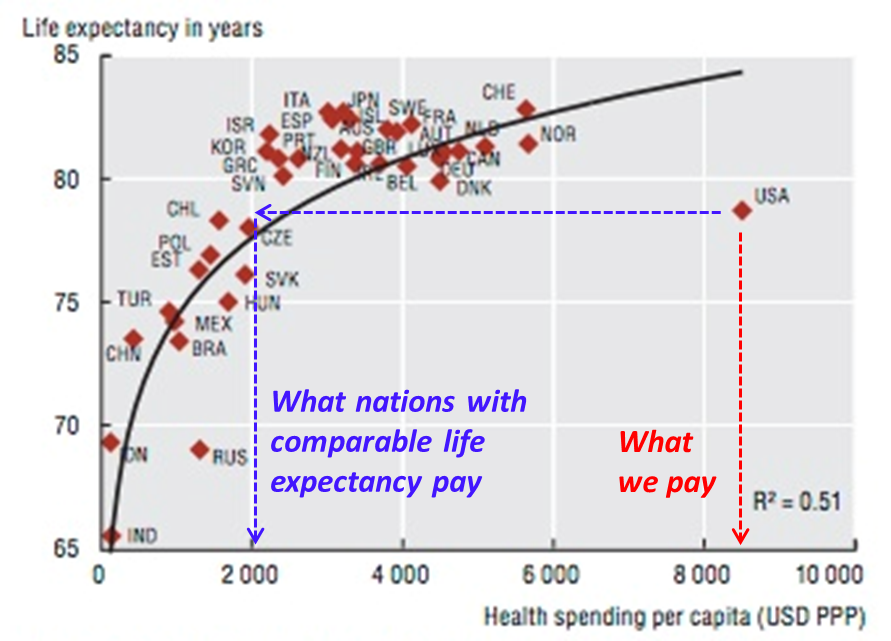
One of the reasons I’m lukewarm about the ACA is that I don’t see it doing much to change the status quo.
UPDATE: I know, health care costs aren’t growing as rapidly as was between ca. 1987 and 2003 but a) they’re still growing several percent above inflation, b) is it sensible for us to be paying 18% of GDP for health care? and c) are we really twice as well off as we were 30 years ago when we were paying about half that? Questions b and c aren’t rhetorical. Are we getting good value? What’s the “opportunity cost” associated with paying so much for health care? Could we have been doing more constructive things with those dollars?
Notes:
- Figuring it ends up getting properly implemented, it’ll almost certainly be an improvement over the status quo. “Improvement over the status quo” is setting the bar pretty low though. Near-universal coverage is good. Lack of mechanisms for bringing cost in line with other advanced nations looks like a problem to me.
- Watch FRONTLINE’s “Sick Around the World” to see how some other advanced nations do health care.
UPDATE 12/15/2013:
Scott Lemieux commentary, BREAKING! The American Political System Does Not Inherently Gravitate Towards Optimal Policy, points out the (obvious) legislative barriers to implementing single payer or any other major policy reform. We have a president not a PM or a dictator.